PTSD, CTE, and Pain Treatment for Veterans is a specialty service available at The Redwood Clinic and with Dr. Jay Sordean. Post-Traumatic Stress Disorder, Chronic Traumatic Encephalopathy, and PAIN are major results of the activities of soldiers not only in battle but in training and even desk jobs. With over 40 years clinical experience in treating these, Dr. Jay Sordean, LAc, OMD, QME has specialized skills that you will not find elsewhere. Call the office today to find out if working together might be helpful. 510-849-1176.
PTSD, CTE, and Pain Treatment for Veterans
<img alt=”Proudly Caring for Veterans Web Badge 600×200″ src=”http://cms-qa.triwest.com/globalassets/vapc3-provider-files/resources/proudlycaringforveterans-horizbadge-600×200.png” height=”200″ width=”600″ border=”0″ />
PTSD, CTE, and Pain Treatment for Veterans
Dr. Jay Sordean’s bestselling book Super Brain: Maximize Your Brain Health for a Better Life is a great place to start to learn more about your brain and the unique approaches used to return your brain to optimal functioning. Https://superbrain-thebook.com
<img alt=”Proudly Caring for Veterans Web Badge 225×300″ src=”http://cms-qa.triwest.com/globalassets/vapc3-provider-files/resources/proudlycaringforveterans-vertbadge-225×300.png” height=”300″ width=”225″ border=”0″ />
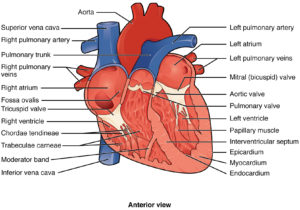
Cardiovascular Disease (CVD) – Natural Medicine Approaches
There is so much more than just pump, wires, and tubes related to your heart — emotions and connections with other people and the world is equally important in heart health.
Cardiovascular disease (CVD) is the number one cause of death in the world. The greatest unnecessary disease of our time, the World Health Organization estimates that ever second death globally is cardiovascular in men and women.
As Michael Gaeta states, “CVD is essentially a deficiency condition. In nearly every person it is an unnecessary, preventable and reversible lifestyle-based condition. Improvements in nutrition, physical activity and social/relational health are safer and more effective than pharmaceutical interventions.” Thus, it is important to avoid the crisis intervention health care system that dominates American medicine.
If you have a desire to reduce the risk factors for CVD using a more natural medicine approach, call us at 510-849-1176 for a consultation.
Heart attacks kill 50% of the people who have them on the first time. Those who survive may have severe reduction in their capacity to exert and function after that. If someone is treated with the proper nutrient combinations after the onset of that low functioning, it is possible to turn around the condition, rebuild the heart function, and improve the activity level of the person who had the heart attack. There are examples of patients who have extreme exertional fatigue, are given only a few months to live. Diligent taking a combination of specific herbs, like hawthorne and garlic, among other important foods, resulted in a patient (with a 6 weeks left to live diagnosis) being out doing intense mountain biking 8 months later.
Your heart will show the condition of the whole body and the nutrition of your entire body systems. It will take the nutrients from the body before other organs and muscles and glands do. So the condition of the heart, when it is studied, will predict other aspects of bodily help. The future of your body. So get your heart checked out the right way and then take serious action.
Call us at 510-849-1176 for a consultation.
Carrageenan: A Dangerous Food Additive to Avoid
Guest Author: Ronald Grisanti D.C., D.A.B.C.O., D.A.C.B.N., M.S., CFMP
Read the labels on the foods you buy.
Watch out for the ingredient carrageenan.
Carrageenan is considered a harmless food additive by the US government.
Unfortunately medical research has proven otherwise.
Carrageenan is known as Irish Moss and is actually a seaweed.
Most people would assume that this food additive would be nutritious considering it is a sea vegetable. On a positive note this sea vegetable is high in iodine, sulfur, trace minerals and vitamins.
But it is important to know that the bad far outweighs the good when it comes to the consumption of carrageenan.
In over 40 studies, carrageenan was found to create ulcers and cancers in animals. It easily triggers inflammatory disease in the human colon as well. And many researchers believe that it promotes not only irritable bowel but breast cancers and more.
It changes detoxification in sulfur pathways (needed for hormones, toxins, etc.,), and may even be responsible for DVT (deep vein thromboses or blood clots in the lower legs).
Chemists have discovered that carrageenan suppresses gamma interferon, a cytokine crucial for tumor and infectious control (like hepatitis), as well as control of inflammation and autoimmune disease, arthritis, and more.
Finally carrageenan has been found to be part of the cause of the epidemic of diabetes, insulin resistance, metabolic syndrome, and more.
The average intake of carrageenan for most individuals is 100 mg a day.
Where do you find carrageenan?
It prevents separation in foods containing milk or chocolate, and improves the texture of not only foods, but cosmetics and even toothpastes, room deodorizers and pesticides.
It’s commonly found in cottage cheese and ice cream to infant formulas, dietetic beverages and low-fat meats and yogurts. For decades it was used as a thickener in puddings.
So the take-away is read the labels on the foods and products you consume and stay clear of anything that has carrageenan listed.
Tobacman JK, et al, Review of harmful gastrointestinal effects of carrageenan in animal studies, Environ Health Persp 109; 10, 2001
Tobacman JK, et al, Carrageenan induces interleukin-8 production through distinct Bc110 pathway in normal human colonic epithelial cells, Am J Physiol, 292: G829, 2006
Suzuki F, et al, Suppression of interferon gamma production in mice treated with carrageenan, Eur J Immunol 16; 4:375-80, 1986
Thompson AW, et al. Immunopharmacology of the macrophagetoxic agent carrageenan, Int J Immunol Pharmacol 1:247-61, 1979
Bhattachryya S, et al, Exposure to the common food additive carrageenan leads to glucose intolerance, insulin resistance, inhibition of insulin signaling…, Diabetologia 55; 1:194-203, 2012
Tomioka H, et al, Comparative roles of macrophages and NK cells in the host resistance of mice to Mycobacterium fortuitum infection, J Infect 48:74-80, 2004 (In this study the investigators found that 3 out of 4 infected mice given carrageenan died of infection)
McKim JM, et al, Food additive carrageenan Part I: A critical review of carrageenan in vitro studies, potential pitfalls and implications for human health and safety, Crit Rev Toxicol 44; 3:211-43, 2014
Yang B, et al, Exposure to common food additive carrageenan leads to reduced sulfatase activity…,Biochimie 94; 6:1309-16, 2012 (and it changes heparin-heparan sulfate disaccharides; does this mean it could lead to deep vein thromboses and lung clots?)
Duarte DB, et al, Models of inflammation: Carrageenan air pouch, Current Protocols Pharmacology, chap 5, unit 5, 6, 2012 (PMID 2278300, carrageenan is used to create inflammation to study NSAIDs)
Gong D, et al, Phytother Res 26; 3:397-402, 2012 (carrageenan is used to create arthritis for animal studies
The information on this website is not intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice. It is intended as a sharing of knowledge and information from the research and experience of Dr. Grisanti and his functional medicine community. Dr. Grisanti encourages you to make your own health care decisions based upon your research andin partnership with a qualified health care professional. Visit FunctionalMedicineUniversity for more information on their training in functional medicine.
Contact Dr. Jay Sordean, LAc, OMD, QME for an appointment for your functional medicine evaluation appointment.
What You Need to Know by guest author
Ronald Grisanti D.C., D.A.B.C.O., D.A.C.B.N., M.S.
[Editor’s Note: I have been teaching this for decades and it is one of the key factors I mention in all of my television appearances as a medical expert]
Many of you reading this short article already know that hemoglobin A1C is extremely useful revealing what the “average” blood sugar has been over the previous ninety days.
This is the same standard laboratory measurement used to measure blood sugar control in diabetics.
What many people may not be aware of is the fact that hemoglobin A1C has important implications for your brain health.
In a landmark study published in the journal Neurology, the researchers documented that elevated hemoglobin A1C is associated with changes in brain size.
The study showed researchers looking at MRIs to determine which lab test correlated best with brain atrophy and found that the hemoglobin A1C demonstrated the most powerful relationship.
They commented, “when comparing the degree of brain tissue loss in those individuals with the lowest hemoglobin A1C (4.4 to 5.2) to those having the highest hemoglobin A1C (5.9 to 9.0), the brain loss in those individuals with the highest hemoglobin A1C was almost doubled during a six-year period.
Is Your Brain Shrinking?
Hemoglobin A1C and Brain Atrophy
Hemoglobin A1C and Brain Atrophy
This profound study strongly indicates that hemoglobin A1C is far more than just a marker of blood sugar balance.
The good news is in most cases you have absolute control over your A1C.
An ideal hemoglobin A1C would be in the 4.8 to 5.4 range. Keep in mind that reducing carbohydrate ingestion, weight loss, and physical exercise will ultimately improve insulin sensitivity and lead to a reduction of hemoglobin A1C.
Dr. Jay Sordean has studied and practiced functional medicine for the last 3 decades. His lectures on the subject can be found on youtube. If you are interested in studying functional medicine, click on this link to FMU76. Compliments from Functional Medicine University
#Alzheimer’s #Dementia #SuperBrain-TheBook #OutsmartingDementia
The Gut Microbiome and Its Potential Role in Obesity is a very hot topic nowadays. Of course the role of the little critters in your intestines (what “gut microbiome” means) is a topic we have discussed here numerous times over the past many decades. Nevertheless, it is good to reexplore the topic repeatedly in relationship to obesity, the gut-brain connection, and the gut-allergy and gut-autoimmune context. This blog is a shortened version of an article from a supplement company and thus the commercial references are not necessarily the choices that Dr. Jay Sordean would use and suggest for you. Call 1-501-849-1176 for your own individual needs.
Source: Journal of Restorative Medicine, Volume 6, Number 1, 6 December 2017, pp. 46-52(7)
Author:Borek, Carmia
ABSTRACT
Obesity has become a major health problem due to its increasing prevalence and its association with chronic disorders that include type 2 diabetes, atherosclerosis, cardiovascular disease, and cancer. Although obesity is a result of a long-term imbalance between dietary intake and energy expenditure, dietary-induced alterations in the gut microbiome play an important role in the onset and development of this condition. Human and animal intestines contain trillions of microbes, defined as the gut microbiome or microbiota. The microbiome is largely responsible for the health of the host and varies with diet, host genotype, sex, and age. The normal gut microbiome imparts specific functions in host metabolism, including immunity, maintenance of the intestinal barrier, and protection against pathogens. The composition and activities of the microbiome are altered in obese individuals compared with their lean counterparts. Metabolic changes due to the altered microbiome in obesity include enhanced energy extraction from food, lipogenesis, and insulin resistance. Dietary manipulation of the microbiome to control obesity includes prebiotics, probiotics, and synbiotics that have been reported to reduce energy storage and lower inflammation and insulin resistance. The development of therapeutic approaches to prevent and treat obesity by microbiome manipulation are being pursued in laboratories and are of growing interest to commercial companies and governments.
INTRODUCTION
Humans and other vertebrates are colonized by a wide array of microbes, collectively called the microbiota or microbiome, terms that define the microbiota genome.
It is estimated that the distal gut contains 10–100 trillion microbes encoding 100 times more genes than the human genome and playing a role in health and disease.
A disturbed microbiome due to altered health or environmental factors may increase the risk of infections and metabolic disorders, including obesity, insulin resistance, diabetes, dyslipidemia, high blood pressure, and cardiovascular disease.
The role of the microbiome in obesity was noted by observing that germ-free mice lacking a microbiome are leaner than conventionally bred mice. The introduction of the gut microbiome from conventionally bred mice into germ-free mice (a process called conventionalization) produced a rapid 60% increase in body fat within 14 days despite a lower intake of chow, normalizing adiposity to the levels of conventionally raised mice.
The leaner state of mice that lacked a microbiome was attributed to their inability to ferment polysaccharide-rich food to the short-chain fatty acids that are a source of energy and lipogenesis. Transferring the microbiome from the conventional mice to the germ-free mice reversed the situation, increasing adiposity and insulin resistance
The ability to transfer the obese or lean phenotype to germ-free mice by means of the microbiome was further observed in a study using the microbiome of human female twins divergent in obesity. Gut microbiome harvested from the obese twin and transferred via gavage to germ-free mice on a low-fat diet resulted in the mice becoming obese; mice colonized with the microbiome from the lean twin remained lean.
EFFECTS OF DIET
Diet modification of the gut microbiome influences obesity.The effect is rapid, with a high-fat diet changing the microbiome within a single day. Diet-induced changes are selective. A Western diet that is high in both fat and sugar correlates with an increased proportion of Firmicutes microbes, which are efficient in harvesting energy from food, over the less efficient Bacteroidetes, potentially leading to obesity. The harvested energy is generated from otherwise indigestible polysaccharides fermented by microbiome enzymes that are not encoded in the human genome. Fermentation products include monosaccharaides and short-chain fatty acids that are absorbed into the circulation, stimulating synthesis of triglycerides in the liver and their incorporation into adipocytes or acting as regulatory molecules.
The main short-chain fatty acids produced by the microbiome are acetate, butyrate, and propionate. Among the three, butyrate and propionate are predominantly antiobesogenic, whereas acetate shows more obesogenic potential. Acetate is oxidized by skeletal and cardiac muscle and by brain cells to carbon dioxide and other metabolites and by adipocytes for lipogenesis, wherein lies its obesogenic potential. Butyrate is metabolized to ketone bodies that provide energy to the colon epithelium. Butyrate improves insulin sensitivity, has antiinflammatory potential, reduces mucosal inflammation, and strengthens the epithelial barrier against invasion and colonization of pathogens, an important function because the disruption of the ecological equilibrium in the gut (i.e. dysbiosis) due to a weakened barrier has been associated with obesity and its related comorbidities.
Propionate has been found to inhibit cholesterol synthesis and to inhibit the expression of resistin,3 an adipocyte-derived signaling polypeptide implicated in obesity-mediated insulin resistance. Furthermore, butyrate and propionate help regulate weight by stimulating anorexogenic gut hormones, which promote a decrease in food intake.
Most studies on the effects of short-chain fatty acids on metabolism, including obesity, have been done with rodents and have often produced contradictory results. Depending on the gut microbiome and the digested food, short-chain fatty acids may have different metabolic effects, resulting in reduced as well as increased obesity.11
Studies with humans show that gut differences and diet affect the microbiome and energy balance.12–16 For example, individuals prone to obesity may harbor a gut microbiome that transports monosaccharaides more efficiently and executes more effective extraction and storage of energy from the diet than the microbiome of lean individuals. In a study addressing the relationship between diet modification of the microbiome and adiposity, 12 obese people were assigned for 1 year to a low-calorie diet that was either fat-restricted or carbohydrate-restricted. A genetic analysis of stool samples showed that 70% of the microbial species were unique to each person and remained constant over time, with members of the Bacteroidetes and Firmicutes divisions dominating the microbiome.12 Obese people had fewer Bacteroidetes and more Firmicutes than did lean control subjects. Weight loss increased the proportion of Bacteroidetes over Firmicutes, regardless of diet type.10,13 In another study with 12 lean and 9 obese people consuming diets that varied in caloric intake (2400 vs. 3400 kcal), researchers found that a higher caloric intake that increased body weight was directly related to a 20% increase in Firmicutes and a 20% decrease in Bacteroidetes.16
INFLUENCE OF DIET CONTENT ON THE MICROBIOME
Changes in diet and lifestyle that began with the introduction of agriculture and animal husbandry are thought to have given rise to alterations in the gut microbiome. Fillippo et al. studied the gut microbiome of children 1–6 years of age from the Mossi ethnic group living in a small village in Boulpon, Burkina Faso (BF), West Africa. The investigators considered the diet of these children as representative of a traditional African diet. They compared the microbiome of the BF children with that of children of the same age living in the urban area of Florence, Italy. The BF children’s diet consisted mostly of millet grain, sorghum (both ground into flour and made into a porridge), and black-eyed peas and other vegetables. The diet was low in calories and high in carbohydrates, fiber, and nonanimal protein. The children from Florence consumed a diet that the investigators considered typical of the Western world, a diet high in fat, animal protein, sugar, and starch but low in fiber. The investigators put forth that the isolation of the BF village where the children lived, compared with urbanized areas, suggested that their diet probably resembled that of the Neolithic populations following the agricultural revolution.17 Using genetic sequencing and biochemical analyses, the researchers in that study found that the BF children had higher levels of Bacteroidetes and lower levels of Firmicutes than the Florentine children, implying that the microbiome of the BF children had coevolved with a high consumption of low-calorie, fiber-rich diets and that the microbiome of the Florentine children was modified by the high-fat and high-sugar diet that could potentially predispose them to future obesity.17
CHILDHOOD MICROBIOME IN RELATION TO LATER OBESITY
The prevalence of certain microbiome species in early childhood may be linked to overweight and obesity in later life.18 Normal-weight infants aged 6 and 12 months showed higher levels of bifidobacteria than children of the same ages who developed obesity at the age of 7 years. Breastfeeding played a determining role in the microbiome composition and in lowering the propensity to obesity in later life.18 Bifidobacteria, especially Bifidobacterium breve,B. infantis, and B. longum, typically colonized the gut microbiome of healthy breastfed infants, reducing the risk of these children being overweight or obese in childhood by 13%–22%. The longer an infant was breast-fed, the lower the likelihood of later-life obesity.18
ARTIFICIAL SWEETENERS AND OBESITY
Artificial sweeteners consumed to combat weight gain may contribute to obesity by altering the microbiome and inducing metabolic changes associated with the metabolic syndrome.19 Mice fed saccharine, sucralose, or aspartame for 11 weeks showed glucose intolerance, compared with control mice fed glucose or sucrose, which remained glucose tolerant. Saccharine exerted the most profound effect and was used in further studies as the prototype sweetener. A high-fat diet induced glucose intolerance in mice fed saccharine but not in control mice fed glucose. Antibiotic treatment that killed the microbiome prevented glucose intolerance. Feces transplanted from glucose-intolerant, saccharine-fed mice to germ-free mice induced glucose intolerance in the germ-free mice, suggesting that metabolic derangements that occurred following the intake of the artificial sweetener were mediated by the gut microbiome.
In a human study, long-term intake of saccharine by 381 individuals without diabetes (44% males, 56% females) correlated with weight gain and a higher fasting glucose level.19 In a prospective study, healthy volunteers (five males and two females, ages 28–36 years) who had not used artificial sweeteners consumed the U.S. Food and Drug Administration maximal daily accepted dose of commercial saccharine (5 mg/kg body weight) for 5 days. Most (four of seven) of the volunteers showed glucose intolerance within days after saccharine consumption. Three were nonresponders and remained glucose-tolerant after saccharine consumption, indicating differences in human metabolic responses to the artificial sweetener. The responders showed pronounced changes in their microbiome, whereas nonresponders had few alterations. Taking stool from responders before and after saccharine consumption and transferring it into germ-free mice resulted in a changed microbiome and glucose intolerance only in the mice given stool from the saccharine consumers, taken after saccharine consumption. By contrast, mice that received stool from nonresponders displayed normal glucose tolerance and an unchanged microbiome.19
These studies suggest that using certain sugar substitutes to prevent obesity may potentially increase the risk of obesity in some people by altering the gut microbiome and inducing metabolic changes associated with obesity. Responses and the final outcome, however, are individualized, driven by personal differences in the microbiome and the possibility of its modification by a particular sweetener.
DIETARY MANIPULATION OF THE GUT MICROBIOME
PREBIOTICS
Prebiotics are nondigestible foods that stimulate the growth and/or activity of colonic microbes.20–27 They offer a safe means of modulating the gut microbiome with a potential to improve host–bacterial interactions in obesity.21,22 Prebiotics alter the microbiome, predominantly by increasing the concentration of bifidobacteria.25,26 The reported metabolic changes that take place include a reduction in hepatic cholesterol and triglyceride, a lowering of inflammation markers,23 enhanced satiety,24 and reduced body fat in children with obesity.26 Volunteers ingesting the fructooligosaccharide inulin at 10 g/day for 16 days showed an increase in Bifidobacterium adolescent from 0.89% at baseline to 3.9%.25
PROBIOTICS
Probiotics are live bacteria and are found in yogurt, kefir, fermented cheese, and standardized supplements. Probiotics modulate the microbiome, but in contrast to prebiotics, they persist for short periods after intake and do not become permanent members of the microbiome.28
Animal and human studies provide evidence that selective probiotics may help prevent adiposity.29–31 Investigators tested the effects of a proprietary probiotic formula on weight control, using the probiotic supplement VSL#3 that contains eight strains of live bacteria: Streptococcus thermophilus,B. brevi, B. longum, B. infantis, Lactobacillus acidophilus, L. plantarum and L. paracasei. In the study, 20 nonobese healthy young males consumed a high-fat diet for 2 weeks, with 10 given VSL#3 and the other 10 a placebo. The probiotic-treated males gained less weight than those on placebo.29
Selective Probiotics May Promote Weight Gain
Probiotics have been used in agriculture to promote the growth of farm animals. Under certain circumstances, selected microbes may similarly affect humans by modifying the microbiome.32High levels of certain intestinal lactobacilli can increase weight and hyperglycemia in healthy adults, though the effects are strain- and dose-specific. Both the bacterial strain and the host are important in determining whether a probiotic preparation will play a role in inhibiting or promoting weight gain, and it is possible that certain marketed probiotics may contain strains that favor obesity. Lactobacillus acidophilus intake, as well as L. fermentum and L. ingluviei, were associated with weight gain in humans and animals, whereas intake of L. gasseri or L. plantarumby obese humans and animals resulted in weight loss.32,33 Because most commercial probiotic preparations include Lactobacillus strains, it may be advisable to monitor the strains of Lactobacillus in the preparation.
Probiotics may be targets for phage infection. So far, there has been limited scientific interest in the identification of phages specific for probiotic bacteria. New methods are needed to prevent or limit the potential negative effects of phage infections on probiotic cultures.34
ALTERING THE MICROBIOME BY SYNBIOTICS AND FECAL TRANSPLANTS
Synbiotics that combine prebiotics and probiotics support the survival of probiotic strains by providing them with prebiotic substrates for fermentation.35 Though in vitro studies have shown that synbiotics are more effective than prebiotics or probiotics in altering the gut microbiome, human studies on the use of synbiotics in treating obesity are limited.36 Fecal transplant from lean to obese persons as a means to treat obesity was reported to increase insulin sensitivity.37 Using this method as an antiobesity treatment requires caution because of the danger of including viral pathogens in the fecal transplant.
CLINICAL CONSIDERATIONS
Diet can selectively modify the composition of the microbiome within 1 day. Both the content of the diet and its caloric value are critical. High-fat diets or diets rich in calories from carbohydrates increase the proportion of Firmicutes over Bacteroidetes, stimulating lipogenesis and weight gain. A hypoenergetic (either low-carbohydrate or low-fat) diet increases the proportion of Bacteroidetes over Firmicutes in parallel with weight loss. The source of fat is important. As seen in animals, saturated fats have different effects on the gut microbiome; a changed microbiome following a feeding of unsaturated fats can protect against weight gain induced by saturated fat.6
A small number of trials have shown that modifying the diet by prebiotics, probiotics, or synbiotics reduces metabolic markers associated with obesity.31,35 Large prospective studies are needed to provide conclusive answers. Prebiotics such as inulin alter the microbial composition. Probiotics must be taken regularly for an effect because the microbes do not become permanent populations in the gut. Different sources of probiotics vary in the types and counts of microbial species. Consequently, they may increase or decrease weight, depending on their content of microbial species and the receiving host.32,33 More studies are needed to identify and promote the growth of gut microbes that would be most effective in reducing obesity.
The ingestion of selected artificial sweeteners has been shown to increase markers of the metabolic syndrome and obesity by disrupting the microbiome.19 The effects in humans were rapid. In a small prospective study, people consuming high doses of saccharin showed insulin resistance after only 5 days. An important point was the fact that the responses varied, with some individuals unaffected by the artificial sweetener.19 These unexpected results on the role of artificial sweeteners in weight gain must be confirmed in larger human studies.
POTENTIAL FUTURE DIRECTIONS
Fighting obesity by regulating the gut microbiome is of growing interest to researchers, commercial companies, and governments. Biotechnology companies are already investing hundreds of millions of dollars in developing a drug based on the human microbiome that will transform the medical treatment of obesity. The White House announced a National Microbiome Initiative in May 2016 to support collaborations between the public and private sectors in developing technologies to generate insight into and expand education on the microbiome.
A greater understanding of the relationships among diet, age, sex, and the microbiome, including host–microbe and microbe–microbe interactions, as well as the modifying effects of specific prebiotics and probiotics, will be crucial in developing a remedy to help control obesity.38Approaches may include identifying foods that affect microbiome genes in relation to obesity and elucidating communication pathways between the gut microbiome and the satiety center in the brain. In summary, a combination of cutting-edge techniques and well-designed human studies are necessary to unravel some of the complexities associated with the microbiome, human genetics, and lifestyle, as well as to help remedy the growing global problem of obesity.
COMPETING INTERESTS
The author declares she has no competing interests.
REFERENCES
Sirisinha S. The potential impact of gut microbiota on your health: current status and future challenges. Asian Pac J Allergy Immunol. 2016; 34:249–64.
Morowitz MJ, Carlisle E, Alverdy JC. Contribution of intestinal bacteria to nutrition and metabolism in the critically ill. Surg Clin North Am. 2011; 9:771–85.
Chakraborti CK. New found link between microbiota and obesity. World J Gasterointest Pathophysiol. 2015; 6:110–9.
Arora T, Bäckhed F. The gut microbiota and metabolic disease: current understanding and future perspectives. J Intern Med. 2016; 280:339–49.
Fändriks L. Roles of the gut in the metabolic syndrome: an overview. J Intern Med. 2017; 281:319–36.
Sonnenburg JL, Bäckhed F. Diet-microbiota interactions as moderators of human metabolism.Nature. 2016; 535:56–64.
Bäckhed F, Ding H, Wang T, et al. The gut microbiota as an environmental factor that regulates fat storage. Proc Natl Acad Sci USA. 2004; 101:15718–23.
Tilg H. Obesity, metabolic syndrome, and microbiota: multiple interactions. J Clin Gastroenterol.2010; 44(Suppl 1):S16–8.
Ridaura VK, Faith JJ, Rey FE, et al. Gut microbiota from twins discordant for obesity modulates metabolism in mice. Science. 2013; 341:1241214.
Ley RE, Bäckhed F, Turnbaugh P, et al. Obesity alters gut microbial ecology. Proc Natl Acad Sci USA. 2005; 102:11070–5.
Ley RE, Turnubaugh PJ, Klein S, Gordon JI. Microbial ecology: human gut microbes associated with obesity. Nature. 2006; 444:1022–3.
Byrne CS, Chambers ES, Morrison DJ, et al. The role of short chain fatty acids in appetite regulation and energy homeostasis. Int J Obesity. 2015; 39:1331–8.
Turnbaugh PJ, Ley RE, Mahowald MA, et al. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature. 2006; 444:1027–31.
Carmody RN, Gerber GK, Luevano JM Jr, et al. Diet dominates host genotype in shaping the murine gut microbiota. Cell Host Microbe. 2015; 17:72–84.
Le Chatelier E, Nielsen T, Qin J, et al. Richness of human gut microbiome correlates with metabolic markers. Nature. 2013; 500:541–6.
Jumpertz R, Le DS, Turnbaugh PJ, et al. Energy-balance studies reveal associations between gut microbes, calorie load, and nutrient absorption in humans. Am J Clin Nutr. 2011; 94:58–65.
De Filippo C, Cavalieri D, Di Paola M, et al. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proc Natl Acad Sci USA. 2010; 107:14691–6.
Kalliomäki M, Collado MC, Salminen S, Isolauri E. Early differences in fecal microbiota composition may predict overweight. Am J Clin Nutr. 2008; 87:534–8.
Suez J, Korem T, Zevi D, et al. Artificial sweeteners induce glucose intolerance by altering gut microbiota. Nature. 2014; 514:181–6.
Delzenne NM, Neyrinck AM, Bäckhed F, Cani PD. Targeting gut microbiota in obesity: effects of prebiotics and probiotics. Nat Rev Endocrinol. 2011; 7:639–46.
Gibson GR, Roberfroid MB. Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. J Nutr. 1995; 125:1401–12.
Floch MH. Probiotics and prebiotics. Gastroenterol Hepatol (NY). 2014; 10:680–1.
Fernandes R, do Rosario VA, Mocellin MC, et al. Effects of inulin-type fructans, galacto-oligosacchrides and related symbiotics on inflammatory markers in adult patients with overweight or obesity: a systematic review. Clin Nutr. 2016; 26:1197–206.
Roberfroid M, Gibson GR, Hoyles L, et al. Prebiotic effects: metabolic and health benefits. Br J Nutr. 2010; 104(Suppl 2):S1–63.
Ramirez-Farias C, Slezak K, Fuller Z, et al. Effects of Inulin on the human gut microbiota: stimulation of Bifidobacterium adolencentis and Faecalibarterium prausnitzii. Br J Nutr. 2009; 101:541–50.
Nicolucci AC, Hume MP, Martínez I, et al. Prebiotic reduces body fat and alters intestinal microbiota in children with overweight or obesity. Gastroenterology. 2017; 153:711–22.
Kumar SA, Ward LC, Brown L. Inulin oligofructose attenuates metabolic syndrome in high- carbohydrate high-fat diet-fed rats. Br J Nutr. 2016; 116:1502–11.
Corthésy B, Gasins HR, Mercenier A. Cross-talk between probiotic bacteria and the host immune system. J Nutr. 2007; 137(3 Suppl 2):781S–90S.
Orterberg KL, Boutagy NE, McMillan RP, et al. Probiotic supplementation attenuates increase in body mass and fat mass during high fat diet in healthy adults. Obesity. 2015; 23:2364–70.
Chen J, He X, Huang J. Diet effects in gut microbiome and obesity. J Food Sci. 2014; 79:R442–51.
Aronsson L, Huang Y, Parini P, et al. Decreased fat storage by Lactobacillus paracasei is associated with increased levels of angiopoietin-like protein (ANGPL4). PLoS One. 2010; 5:e13087.
Million M, Angelakis E, Armougom F, et al. Comparative meta-analysis of the effect of Lactobacillus species on weight gain in humans and animals. Microb Pathog. 2012; 53:100–8.
Million M, Lagier JC, Yahav D, et al. Gut bacterial microbiota and obesity. Clin Microbiol Infect.2013; 19:305–13.
Ventura M, Sozzi T, Turroni F, et al. The impact of bacteriophages on probiotic bacteria and gut microbiota diversity. Genes Nutr. 2011; 6:205–7.
Vitali B, Ndagijmana M, Cruciani F, et al. Impact of symbiotic food on the gut microbial ecology and metabolic profiles. BMC Microbiol. 2010; 10:4.
Beserra BT, Fernandes R, do Rosario VA, et al. A systematic review and meta-analysis of the prebiotic and synbiotic effects on glycemic, insulin concentration and lipid parameters in adult patients with overweight or obesity. Clin Nutr. 2015; 34:845–58.
Smith LP, Bouter KE, deVos WM, et al. Therapeutic potential of fecal microbiota transplantation.Gastroenterology. 2013; 145:946–53.
Portune KJ, Benítez-Páez A, Del Pulgar EM, et al. Gut microbiota, diet and obesity related disorders-the good, the bad, and the future challenges. Mol Nutr Food Res. 2017; 61:1600252. doi: doi: https://doi.org/10.1002/mnfr.201600252.
An increasing body of scientific and clinical evidence show that brain health needs personalized and multi-pronged interventions to optimize health outcomes. Nutrition and cognition (thinking) are linked. More and more researchers are offering links demonstrating how poor nutritional intake adversely affects cognitive functioning and may, in fact, contribute to various neurological conditions including anxiety, depression, autism and neurodegenerative disorders. Data are indicative that these links may begin before birth, continue throughout the life course and be particularly susceptible during times of inadequate or inappropriate nutritional intake, physiological changes or increased stress.
Many scientific sources confirm evidence of the gut-brain axis, its association to nutrition, and how it influences cognitive health throughout life—from birth into later years. These include:
-The links between stress, chronic inflammation, nutrition and cognitive health
-The critical role nutrition plays in gut and neurological health
-How to leverage specific nutritional solutions to optimize gut-brain outcomes for health conditions
Dr. Jay Sordean talking about Stress and Managing Stress on KREM2 Spokane with Rose Beltz, Health News Reporter.
Stress and Stress Management, Because Stress is Pervasive
Stress is a response to external and internal changes in our environment and how we perceive of it.
We both react and respond to stressful situations.
“Reaction” is more automatic and unconscious.
“Response” is more mediated, less automatic, and tempered by conscious and learned beliefs and behaviors. Response modifies and can reduce a severe stress reaction like panic attacks.
There are several types of stress response and reactions:
• Mental
• Emotional
• Physical
• Spiritual
• Energetic
The deepest basis for our bodily reactions and responses to external and internal changes is our need to survive.
It is both our individual survival and our survival as a family, tribe, and species that drives stress behavior.
The survival stress reaction is called the “Fight or Flight” response. This is deeply seated in our survival brain and is body based. Strong hormones surge through the body and effect breathing, heart rate, digestion, thinking, emotions.
The most common stressors, according to statistics, are:
• Death of a loved one
• Divorce
• Loss of a job
• Increase in financial obligations
• Getting married
• Moving into a new home
• Chronic illness or injury
• Emotional problems (depression, anxiety, anger, grief, guilt, low self-esteem)
Stressful, or even life-threatening situations include:
• Threat of physical harm
• Threat of freezing or of burning up
• Threat to our loved ones (children, parents, family, friends)
• Unhealthy living situation – like mold in a house
• Toxic relationships
• Changes in intimate relationships
• Divorce, break-up, infidelity
• Abusive relationships
• Toxic work environment (chemicals, people, activities)
• Negative self-talk
These are a few of the many solutions to help empower you to become stress-responsive versus simply stress-reactive
• Fixing up dangerous housing environment (mold abatement, getting rid of drug infested nuisance properties, reducing crime statistics with better job opportunities) (contact www.TwinHomeSolutions.com for help if you have bad homes in your neighborhood)
• Learning breathing exercises, visualization exercises, empowerment (like “fist pump”)
• Doing yoga, meditation, Tai Qi, Qi Gong (we can demonstrate that for you)
• Using BANK Code personality typing to communicate better with your loved ones or spouse (go to www.Four-Cards.com to get your free $97 value gift of a personality analysis from Dr. Jay)